Breast Cancer Staging: Physiology Trumps Anatomy
Author: Maxine Jochelson, MD, FSBI
The purpose of this paper is to address the importance of physiologic imaging for the staging and follow up of patients with breast cancer according to the principles of precision medicine. Precision medicine is the “tailoring of medical treatment to the individual characteristics, needs and preferences of a patient during all stages of care, including prevention, diagnosis, treatment and follow-up.” Currently, physiologic imaging is primarily performed with 18F –FDG- PET/CT, but other tracers are increasingly being used towards the goal of more specific tumor targeting.
Staging
Once breast cancer is diagnosed, staging of the axilla must be performed. However, at present, imaging of the clinically negative axilla is not accurate enough to obviate histologic sampling, which is most frequently performed with sentinel lymph node biopsy. Houssami et al. reported in a meta-analysis of 31 studies that axillary ultrasound had a sensitivity of only 61.4%1 . PET/CT provides similar limited sensitivity in the general breast cancer population2; however, in patients with larger primary tumors who may undergo neoadjuvant chemotherapy, sensitivity is 82% for the detection of regional lymphadenopathy reflecting a higher likelihood of nodal metastases in women with larger cancers3. Based on these data Koolet et al recommend that all patients who will be undergoing neoadjuvant chemotherapy have an FDG PET/CT scan for locoregional staging. Current National Comprehensive Cancer Network (NCCN) guidelines recommend against routine staging of women with Stage I or II disease and primarily recommend CT or MRI in addition to a bone scan for staging women with Stage III or IV breast cancer with the following caveat: “The use of FDG PET/CT should generally be discouraged for the evaluation of metastatic disease except in those clinical situations where other staging multiple studies all demonstrating more accurate breast cancer staging with FDG PET/CT as will be briefly described below. In breast cancer detection, it is already well established that physiologic imaging of the breast (with breast MRI, Positron Emission Mammography, Molecular Breast Imaging, and Contrast Enhanced Mammography) has a higher sensitivity than purely anatomic modalities (including Full Field Digital Mammography, Digital Breast Tomosynthesis, and ultrasound).
Groheux et al. evaluated 254 women with Stage IIA through IIIC breast cancer and found that FDG PET/CT imaging changed the clinical stage in 30% of the women. Most strikingly, 21% of those women had unsuspected metastatic disease, with an upgrade rate of 10.7% in women with Stage IIB disease4. In a retrospective study of breast cancer patients younger than 40 years of age, Riedl et al. demonstrated a 17% upstaging rate in women with IIB disease5.
Every study comparing FDG PET/CT to standard imaging with CT and bone scan has demonstrated the superiority of PET/CT with accuracies of 86-90% 6,7. Constantinidou et al.8 compared FDG PET/CT to CT and bone scan and showed more disease in over 30% of patients. Although the finding of additional metastases when a patient clearly has extensive metastatic disease may not always be clinically relevant, there are times when PET/CT detects a single metastases when all other exams are negative changing treatment and prognosis. It should be stressed that in these cases biopsy confirmation is required when possible to avoid overtreatment of a false positive PET/CT finding.
Figure 1 shows PET/CT imaging of a 35-year-old Asian woman presenting with Stage IIB breast cancer who was waiting for the results of BRCA testing to determine if she were to have bilateral mastectomy and reconstruction. PET/CT showed a 6 mm mediastinal node (normal by CT criteria) which was FDG avid. Biopsy proved metastatic disease. Treatment plan was changed from mastectomy to chemotherapy alone.

Figure 1
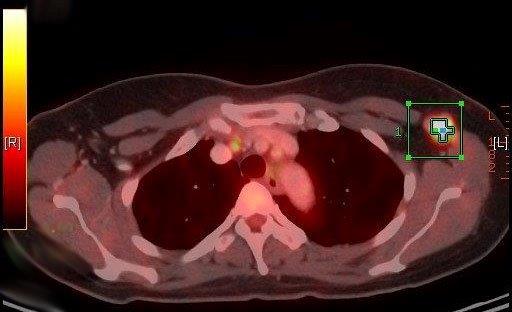
Figure 1B
Despite the overall excellent results obtained with PET/CT for staging, however, its utility is not uniform among all types of breast cancer. Dashevsky et al. evaluated FDG PET/CT for its ability to detect bone metastases in 95 women with invasive lobular carcinoma (ILC). They found that ILC bone metastases were more commonly sclerotic on CT than patients with infiltrating ductal carcinoma (IDC) and infiltrating mammary carcinoma (IMC). The standardized uptake value (SUV) max in patients with ILC was lower than in patients with IDC and in fact only three of seven ILC patients with sclerotic bone metastases had a FDG-positive PET scan 9. In another study, Hogan et al. evaluated 87 patients with ILC and found that PET/CT did not reveal unsuspected extra-axillary nodes in any patient10.
Follow Up
1. Treatment Response
Besides being the most accurate modality for locoregional and systemic staging in breast cancer, 18 F-FDG PET/CT accurately predicts treatment response. As far back as 1993, Wahl et al. reported that patients who ultimately responded to chemotherapy showed a 50% decrease in uptake two months into chemotherapy compared to nonresponders, and this change in uptake was independent of change in size11. Vranjesevic et al. compared the predictive ability of PET/CT to that of conventional imaging in 61 patients and showed that the positive predictive value (PPV) of PET/CT was 93% compared to 85% for conventional imaging, and that the negative predictive value (NPV) was 84% for PET/CT compared to 59% for conventional imaging12. Other (nonFDA approved) PET tracers have also been demonstrated to predict response at an early time point, allowing for potential earlier treatment change (risk adaptive treatment). Kenny et al. used 18F-fluorothymidine (FLT) PET which assesses tumor proliferation and showed that a decrease in SUV at 1 week discriminated between clinical response and stable disease13. Theoretically, if the oncologists can determine that a certain drug combination is not working at an earlier time point, the treatment course may be altered and the patient could benefit from a different treatment before an increase in disease burden which may render the disease more difficult to treat, and avoid unnecessary morbidity of ineffectual therapy. This “risk adaptive” approach has been successful in treating patients with lymphoma and hopefully can be adopted in breast cancer as well. Once a patient has been treated for breast cancer, accurate assessment of treatment response is vital for both clinical trials as well as for patient care. Currently, for clinical trials and in many practices, follow up assessments of patients are often made using purely anatomic imaging, most often with CT scanning. Decrease in the size of the tumor after treatment is the measure of response. This approach is particularly problematic in women with breast cancer since bone is the most common site of metastatic disease and bone metastases cannot be reliably measured unless there is an extraosseous soft tissue mass associated with the bone lesion. Otherwise, it is difficult to determine treatment response. Development of or increase in sclerosis can be due to either healing or progressive disease. Likewise, a bone scan may show increased uptake caused by a metabolic flare, progression, or disease healing.
If PET/CT is employed, physicians will be able to measure the change in SUV reflecting change in metabolic activity and thus determine response to treatment.
Figure 2 shows PET/CT imaging in a patient with known hypermetabolic sclerotic metastasis to L3. After treatment, there were no changes in the appearance on CT imaging; the patient would be considered as having a stable disease. However, on PET/CT imaging, there is a significant reduction in FDG activity, confirming treatment response.
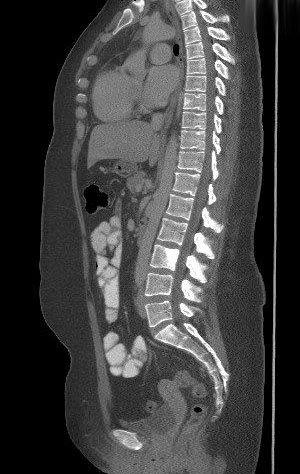
Figure 2A

Figure 2B

Figure 2C

Figure 2D
Figure 3 shows PET/CT imaging in a patient with bone only metastases at presentation and who had a good response to chemotherapy in her bone metastases. However, at the same time as the response in the bone, the patient developed a liver metastasis, which was only seen on FDG PET/CT.
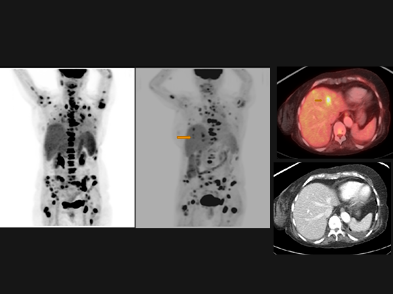
Figure 3
Another source of difficulty when assessing treatment response is that patients often have a heterogeneous response within the various tumor sites. This is of particular concern in women presenting with bone metastases. It is well recognized that even within the same patient, there is tumor heterogeneity14. Huyge et al. demonstrated that in 46 women with bone dominant metastatic breast cancer, the women had heterogeneous response in 43% of the treatment phases; in the subset with both bone and extra-bone metastases, PET/CT showed discordant responses between bone and extra-bone metastases in 30% of treatment phases.15 In a study that did not include FDG PET Lorincz16 evaluated 48 women with metastatic breast cancer and showed that half of those with HER 2+ disease lost the genotype in their bone metastases.
2. Clinical trial evaluation
The treatment response of patients in clinical trials is most often evaluated by CT using the RECIST (Response Evaluation Criteria in Solid Tumors) 1.1 criteria and is therefore purely anatomic. Five lesions are chosen per patient and except for lymph nodes, a single measurement of the longest diameter of the metastasis is followed. For lymph nodes, a measurement of the short axis, which must be at least 1.5 cm, is followed. Reliability of measurements has been called into question. PERCIST (Positron Emission Tomography Response Criteria in Solid Tumors adds physiology to anatomy. FDG PET/CT is performed >10 days after chemotherapy with measurement of up to five lesions with the most intense uptake. Response is defined as the % change in SUL (SUV corrected for lean body mass).
The following case demonstrates the superiority of PERSIST:
Figure 4 shows FDG PET/CT in a 35-year-old woman who presented with lung and liver metastases. As a baseline (Figure 4A) for a clinical trial, she had CT chest, abdomen, and pelvis with contrast as required by protocol which used RECIST 1.1 criteria to assess response. She also had a PET/CT. After the first three months of chemotherapy she was re-imaged (4B) as per protocol and demonstrated complete response in the lung and near complete response in the liver on both CT and PET/CT with a residual small, mildly FDG avid lesion in the posterior right lobe. She therefore qualified for more chemotherapy after which CT was stable by RECIST which meant that she would undergo another two cycles of chemotherapy even though the residual liver lesion had become more hypermetabolic and a new area of FDG avidity had developed in another part of the liver. After the next two cycles of this experimental regimen which was clearly not working by PET criteria, she also demonstrated progression on CT. At that point she was considered to have disease progression and taken off the initial protocol and switched to a different chemotherapy combination:
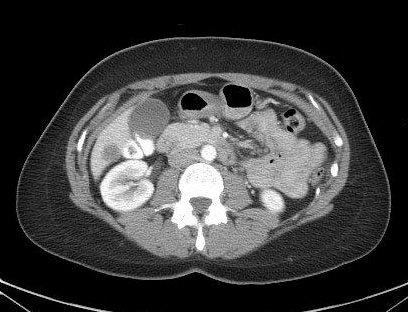
Figure 4A
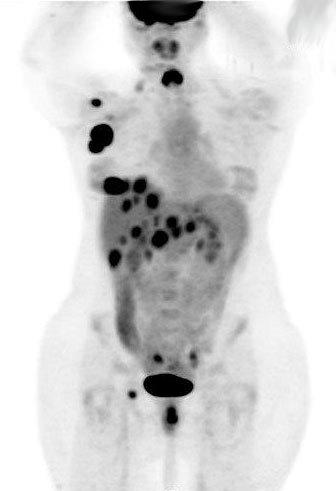
Figure 4A2

Figure 4B

Figure 4B2
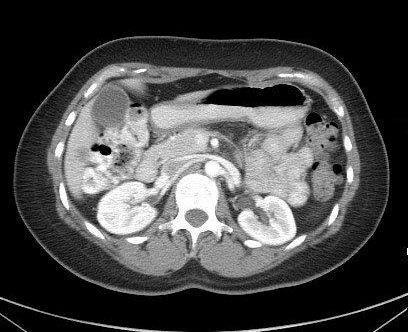
Figure 4C
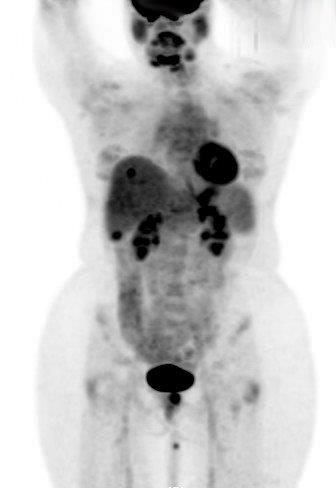
Figure 4C2
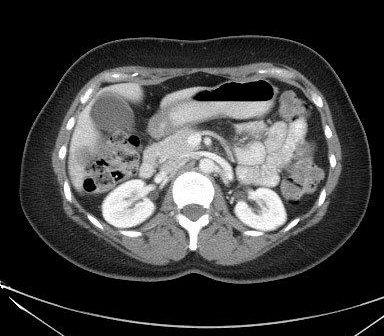
Figure 4D
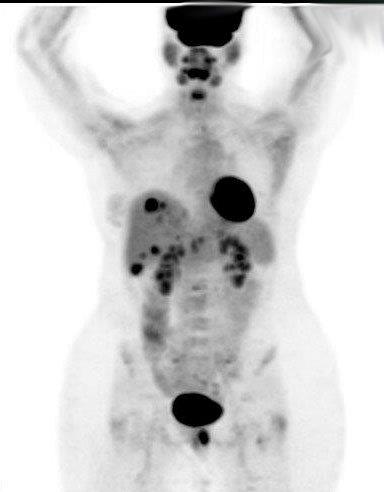
Figure 4D2
There are several reasons why this case is an important example. To begin with, this patient underwent two additional cycles of chemotherapy that was not working. This is not only burdensome for the patient; these drugs can be very expensive--far more costly than the additional cost of a PET scan, and can result in additional side effects. Additionally, since this was done on a clinical trial which evaluated the ability of the drug to improve freedom from progression--an endpoint measured in weeks or months in patients with metastatic breast cancer--the results demonstrated two additional months of freedom from progression by using the CT results which suggested that the chemotherapy regimen being tested had performed better than it actually had, instead of the more accurate PET/CT results which indicated its lack of efficacy.
In a retrospective study, Riedl et al. compared RECIST to PERSIST for their ability to predict progression free survival (PFS) and disease specific survival (DSS) in 71 stage IV patients. PET demonstrated response in patients who had stable CTs and was significantly better at predicting PFS and DSS in these patients17.
Looking forward
Targeted therapy is increasingly being used for various subtypes of breast cancer. At the same time, tumorspecific tracers are being developed including 18F-fluoroestradiol (FES) which targets estradiol and may be superior in some estrogen receptor positive tumors18 and 89Zr-trastuzumab which targets HER 2+ cancers. Although discussion of these tracers is beyond the scope of this paper, it should be noted that the use of new and different tracers should enhance the ability to stage cancer, predict for and assess treatment response beyond the standard imaging with -FDG PET/CT.
Conclusion
In conclusion, physiologic imaging trumps anatomic imaging not only in the detection of breast cancer but also in the staging of breast cancer and evaluation of response to treatment. As we aim to develop more successful and targeted personalized treatment, targeted personalized imaging will play a critical role in optimizing patient care as well as clinical trial evaluation.